How to Choose the Right Atlanta Rehabilitation Center for Your Loved One’s Specific Needs
Originally published: May 2025 | Updated: June 2026 | Reviewed by Sadie Mays
Originally published: May 2025 | Updated: June 2026 | Reviewed by Sadie Mays

Atlanta rehabilitation centers provide physical therapy, occupational therapy, and speech-language pathology to help individuals recover from surgery, stroke, cardiac events, falls, and chronic conditions.
Medicare Part A covers skilled nursing rehabilitation for up to 100 days after a qualifying 3-day hospital stay — with zero copay for days 1 through 20 and a $217 daily coinsurance for days 21 through 100 in 2026, per CMS published rates.
The most important step in choosing a center is matching the facility’s therapy services and clinical staff to the resident’s documented medical, functional, and cognitive needs.
Sadie G. Mays Health & Rehabilitation Center is a 206-bed, 501(c)(3) nonprofit skilled nursing facility in northwest Atlanta, founded in 1947, providing in-house rehabilitative services seven days a week.
Your parents’ hospital is preparing a discharge plan, and you need a rehab facility that provides daily therapy, 24-hour nursing, and a real recovery timeline — the Sadie G. Mays admissions team can confirm bed availability and verify insurance within 24 hours. Call 678-420-2946.
Post-acute rehabilitation is appropriate for any individual who has lost functional ability due to a hospitalization, surgery, injury, or disease progression and needs structured daily therapy under clinical supervision to regain independence.
A physician’s order for skilled nursing rehabilitation specifies the clinical need — this is not a family decision or a lifestyle preference.
Conditions that commonly require inpatient rehabilitation in a skilled nursing facility include:
Families navigating a hospital discharge should ask the discharge planner whether the physician has ordered skilled nursing rehabilitation or home health — the answer determines whether an inpatient facility or an outpatient program is clinically appropriate.
Atlanta families have three rehabilitation delivery models: inpatient rehabilitation inside a skilled nursing facility, outpatient rehabilitation at a clinic, and home-based rehabilitation delivered by a visiting therapist. The correct model depends on the resident’s medical stability, therapy intensity requirements, and level of independence.
| Rehab Delivery Model | Setting | Therapy Intensity | Best For |
| Inpatient (SNF-based) | 24-hour skilled nursing facility | Daily sessions, 5–7 days per week | Post-surgical, post-stroke, medically complex, high fall risk |
| Outpatient | Clinic or hospital-based | 2–3 sessions per week | Medically stable, independent mobility, strong home support |
| Home-based | Patient’s residence | 2–3 sessions per week | Transportation barriers, mobility limitations, mild therapy needs |
Inpatient rehabilitation inside a skilled nursing facility provides daily therapy sessions under 24-hour nursing supervision with physician oversight. Residents receive physical therapy, occupational therapy, and speech-language pathology from licensed therapists on-site — not contracted providers who appear two days a week. Medicare Part A covers this level of care for up to 100 days per benefit period.
Sadie G. Mays provides inpatient rehabilitation with in-house licensed therapists delivering daily sessions seven days a week, coordinated by a geriatric-certified Medical Director and supervised by registered nurses on every shift.
Outpatient rehabilitation serves individuals who are medically stable, mobile enough to travel to a clinic, and able to manage daily activities safely between sessions. Outpatient therapy runs 2 to 3 sessions per week and is covered under Medicare Part B with applicable copays.
Outpatient rehab is appropriate after a short inpatient stay has restored baseline mobility, or for chronic conditions requiring maintenance therapy.
Home-based rehabilitation sends licensed therapists to the patient’s residence — an option for individuals with transportation barriers, severe mobility limitations, or mild therapy needs that do not require daily frequency.
Home-based programs deliver 2 to 3 sessions per week and are covered under Medicare home health benefits when ordered by a physician.
Sadie G. Mays does not provide home-based therapy directly but coordinates discharge referrals to Medicare-certified home health agencies in the Atlanta metro area.
If you’re ready to get started, call us now!
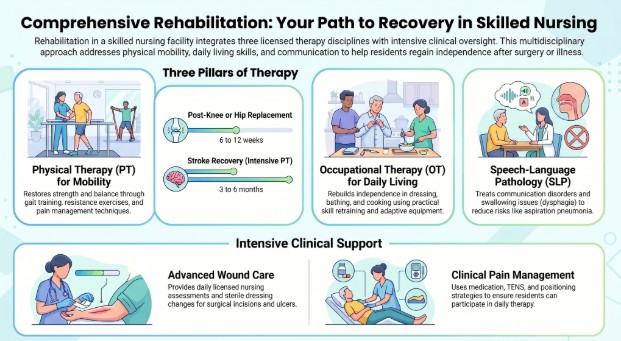
Rehabilitation in a skilled nursing facility combines three licensed therapy disciplines — each addressing a different dimension of functional recovery.
Physical therapists assess and treat movement problems caused by surgery, injury, or disease. PT sessions at a skilled nursing facility include gait training (relearning to walk safely), balance exercises, stair climbing, resistance-band and weight-based strengthening, manual therapy (hands-on muscle and joint mobilization), and pain management techniques, including heat, cold, and electrical stimulation.
Recovery timelines vary by condition. Post-knee or hip replacement patients typically regain functional mobility within 6 to 12 weeks of daily therapy, with many returning to daily routines within 3 months.
Stroke survivors may require 3 to 6 months of intensive PT, per the American Stroke Association. Therapists adjust treatment intensity as patients progress, setting measurable weekly goals documented in the care plan.
Occupational therapists help residents regain the ability to perform activities of daily living independently — dressing, bathing, grooming, cooking, eating, and managing household tasks. OT sessions focus on practical skill retraining, adaptive equipment training (e.g., reachers, sock aids, shower benches), and home safety modifications planned prior to discharge.
For residents with cognitive impairment from stroke, traumatic brain injury, or early-stage dementia, occupational therapists use memory exercises, environmental cues, repetition-based routines, and compensatory strategies to maximize the resident’s functional independence within their cognitive capacity.
Speech-language pathologists treat communication disorders — aphasia, dysarthria, apraxia of speech — that commonly follow stroke, traumatic brain injury, or progressive neurological disease.
SLPs also evaluate and treat swallowing disorders (dysphagia), a condition that affects an estimated 15% of hospitalized older adults and carries significant aspiration pneumonia risk if untreated, per the American Speech-Language-Hearing Association.
At Sadie G. Mays, speech therapy is delivered by licensed SLPs on-site as part of each resident’s individualized rehabilitation plan — not contracted on a limited schedule.
Skilled nursing facilities provide clinical pain management and wound care services that outpatient clinics and home health programs cannot replicate at the same intensity.
Pain management protocols include medication management, transcutaneous electrical nerve stimulation (TENS), therapeutic heat and cold applications, and positioning strategies designed to reduce discomfort, enabling residents to participate fully in daily therapy sessions.
Wound care teams at skilled nursing facilities treat surgical incisions, pressure injuries, diabetic ulcers, and post-operative wound complications — conditions that require daily licensed nursing assessment, sterile dressing changes, and documentation of healing progress.
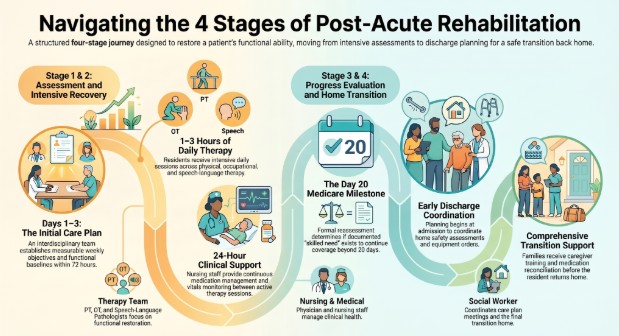
Post-acute rehabilitation in a skilled nursing facility follows four stages, each with a defined clinical purpose and family role.
The interdisciplinary team — attending physician, nursing staff, physical therapist, occupational therapist, speech-language pathologist, and social worker — evaluates the resident’s medical status, functional baseline, cognitive capacity, and rehabilitation goals.
The team produces an individualized care plan with measurable weekly objectives. Families participate in the initial care plan meeting within the first 72 hours of admission.
The resident receives daily therapy sessions — typically 1 to 3 hours per day across PT, OT, and speech — designed to restore functional ability as rapidly as the resident’s medical status allows. Nursing staff monitor vitals, manage medications, and provide 24-hour clinical support between therapy sessions. Families receive progress updates at scheduled intervals.
The care team formally reassesses the resident’s progress against the original goals, adjusts therapy intensity and focus, and determines whether the resident is on track for discharge or requires an extended stay. Medicare requires documented skilled need to continue coverage beyond day 20.
The social worker and therapy team coordinate the transition home — including home safety assessment recommendations, outpatient therapy referrals, durable medical equipment orders, medication reconciliation, and caregiver training.
Sadie G. Mays begins discharge planning at admission, not as an afterthought in the final week.
Recovery timelines depend on the underlying condition, the resident’s baseline health, and the intensity of therapy received. The table below reflects typical ranges for residents receiving daily inpatient therapy at a skilled nursing facility.
| Condition | Typical Inpatient Rehab Duration | Expected Functional Milestone |
| Hip or knee replacement | 10–21 days | Independent transfers and assisted ambulation |
| Hip fracture repair | 14–28 days | Safe walker-assisted mobility |
| Stroke (moderate severity) | 21–60 days | Functional speech, assisted ADLs, supervised mobility |
| Cardiac surgery | 10–21 days | Monitored stair climbing, independent ADLs |
| Major abdominal surgery | 7–14 days | Independent bed mobility and ambulation |
| Parkinson’s or MS exacerbation | 14–30 days | Restored baseline function, fall prevention strategies |
| Falls with injury | 14–28 days | Balance retraining, home safety readiness |
Medicare Part A covers up to 100 days of skilled nursing rehabilitation per benefit period, but the average post-acute stay runs 20 to 30 days.
Residents who plateau — meaning therapy produces no measurable functional improvement over a defined period — may lose Medicare coverage before day 100.
Families should track progress through weekly care plan updates and ask the therapy team directly whether the resident is meeting documented rehabilitation goals.
Your parent just had surgery, and the hospital says rehab could take weeks — the Sadie G. Mays admissions team can walk you through what daily therapy looks like, how long recovery typically takes for the specific condition, and what Medicare will cover. Call 678-420-2946.
If you’re ready to get started, call us now!
A quality rehabilitation center combines proper licensure, experienced clinical staff, individualized care plans, and family involvement. Families evaluating facilities should verify:
Sadie G. Mays is Medicare- and Medicaid-certified and accredited, and it publishes its CMS Care Compare profile for public review. The facility completed a $3.2 million renovation in 2025, covering rehabilitation spaces, dining rooms, and resident rooms.
Coverage rules determine how long a resident can stay and how much the family pays out of pocket.
| Payment Source | What It Covers | Key Conditions (2026) |
| Medicare Part A | Days 1–20: $0 copay. Days 21–100: $217/day coinsurance | Qualifying 3-day inpatient hospital stay; documented skilled need |
| Medicare Part B | Outpatient therapy sessions | 80% of the approved amount after the annual deductible |
| Georgia Medicaid | Long-term skilled nursing after Medicare exhaustion | Income below $2,982/mo; assets below $2,000 (2026 GA DCH thresholds) |
| Long-term care insurance | Varies by policy — typically covers SNF rehab | Benefit trigger: cannot perform 2+ ADLs or cognitive impairment |
| VA Aid and Attendance | Up to $2,424/mo for eligible veterans (2026) | Wartime service; clinical need documented |
| Private pay | Full daily rate | No restrictions |
Medicare Part A requires documented skilled need — meaning the resident must be receiving therapy that produces measurable functional improvement. When a resident plateaus and therapy no longer produces documented progress, Medicare coverage may end before day 100.
Families should understand rehabilitation payment options before admission and ask the facility’s billing team for a written estimate of out-of-pocket costs at each coverage stage.
Families who anticipate a transition from short-term rehab to long-term care should begin Georgia Medicaid planning before day 20 of the Medicare stay — not after coverage lapses.
Three red flags reliably signal a facility that will not meet a resident’s rehabilitation needs:
Lack of transparency. Facilities that avoid direct answers about therapy schedules, staff credentials, cost breakdowns, or inspection results are hiding information families need. A quality center provides documentation on request and encourages facility tours with full access to therapy spaces and resident areas.
Overcrowding and understaffing. Facilities that treat more residents than their staffing can safely manage produce longer wait times for therapy, delayed medical responses, and higher rates of missed sessions. Families should ask for the exact therapist-to-patient ratio and not accept vague assurances.
One-size-fits-all care plans. Facilities that apply the same therapy schedule to every resident regardless of diagnosis, functional baseline, or goals are not providing individualized rehabilitation.
Effective rehab requires a plan built from a clinical assessment, adjusted weekly based on documented progress, and reviewed with the family at regular intervals.
What should families consider when choosing a rehabilitation center in Atlanta?
Families should match the facility’s therapy services to the resident’s documented clinical needs, verify CMS star ratings and Georgia licensure, confirm daily in-house therapy from licensed therapists, and request an itemized cost breakdown before signing an admission agreement.
What is the difference between inpatient and outpatient rehabilitation?
Inpatient rehabilitation provides daily therapy sessions inside a skilled nursing facility with 24-hour nursing supervision. Outpatient rehabilitation delivers 2 to 3 sessions per week at a clinic while the patient lives at home — appropriate for medically stable individuals with adequate home support.
How long does rehabilitation take after hip or knee replacement surgery?
Post-knee or hip replacement patients receiving daily inpatient therapy typically regain functional mobility within 6 to 12 weeks, with many returning to daily routines within 3 months. Individual timelines vary based on the patient’s baseline health, surgical complexity, and participation in therapy.
What is the difference between physical therapy, occupational therapy, and speech therapy?
Physical therapy restores mobility, strength, and balance through exercise and manual techniques. Occupational therapy helps rebuild the ability to perform daily activities such as dressing, bathing, and cooking. Speech-language pathology treats communication disorders and swallowing problems that commonly follow stroke or brain injury.
Does Medicare cover rehabilitation in a skilled nursing facility?
Medicare Part A covers skilled nursing rehabilitation for up to 100 days per benefit period after a qualifying 3-day hospital stay. Days 1 through 20 are fully covered; days 21 through 100 require a $217 daily coinsurance amount in 2026, per CMS-published rates.
Does Sadie G. Mays provide home-based rehabilitation services?
Sadie G. Mays provides inpatient rehabilitation with in-house licensed physical, occupational, and speech therapists. The facility does not deliver home-based therapy directly but coordinates discharge referrals to Medicare-certified home health agencies serving the Atlanta metro area.
What conditions require inpatient rehabilitation in a skilled nursing facility?
Conditions requiring inpatient rehab include hip fracture, knee or hip replacement, stroke, cardiac surgery, spinal surgery, falls with injury, and exacerbation of chronic conditions like Parkinson’s disease or COPD that reduce functional ability below safe independent living thresholds.
How can families verify the quality of a rehabilitation center?
The CMS Care Compare database at medicare.gov publishes star ratings, staffing data, inspection results, and quality measures for every Medicare-certified facility. Families should also verify Joint Commission or CARF accreditation, confirm daily in-house therapy staffing, and review the facility’s most recent state inspection report.
What happens after rehabilitation is complete?
The care team coordinates discharge planning, including home safety recommendations, outpatient therapy referrals, durable medical equipment orders, medication reconciliation, and caregiver training. Facilities that begin discharge planning at admission produce safer transitions than those that wait until the final week.
Are customized rehabilitation care plans available at Sadie G. Mays?
Every resident at Sadie G. Mays receives an individualized care plan developed by the interdisciplinary team — physician, nursing staff, licensed therapists, and social worker — within 72 hours of admission. Care plans are reviewed and adjusted weekly based on documented progress toward measurable functional goals.
Your loved one needs a rehab facility that delivers daily licensed therapy, starts discharge planning on day one, and keeps the family informed at every stage — the Sadie G. Mays admissions team does exactly that for Atlanta families. Call 678-420-2946.