Nursing Home vs. Assisted Living in Atlanta: Which Level of Care Does Your Loved One Actually Need?
Originally published: March 2026 | Reviewed by Sadie Mays
Originally published: March 2026 | Reviewed by Sadie Mays
Data last verified: March 2026
A skilled nursing facility (SNF) is a Medicare- and Medicaid-certified residential care setting that provides 24-hour licensed nursing supervision, physician oversight, and on-site rehabilitation therapy for individuals with complex or post-acute medical needs.
An assisted living community is a state-licensed residential care setting that provides help with activities of daily living — bathing, dressing, meals, and medication reminders — for seniors who are medically stable and do not require around-the-clock clinical oversight.
Selecting the wrong setting creates a measurable safety risk and unnecessary cost. The correct placement is determined by the resident’s documented clinical need, not by age, family preference, or proximity to relatives.
A nursing home — formally designated a skilled nursing facility (SNF) — is a licensed residential care setting that delivers around-the-clock nursing supervision, physician oversight, and clinical rehabilitation services to individuals who cannot be safely managed in a home or lower-acuity care environment.
The Centers for Medicare and Medicaid Services (CMS) certifies skilled nursing facilities as a condition of Medicare and Medicaid reimbursement.
The Georgia Department of Community Health’s Healthcare Facility Regulation (HFRD) division licenses and inspects every skilled nursing facility operating in Georgia.
CMS certification and Georgia HFRD licensure are both required before a skilled nursing facility may bill Medicare or Medicaid for resident care.
Skilled nursing facilities serve two clinically distinct resident populations.
Short-term rehabilitation residents are individuals recovering from a hospitalization — hip fracture repair, stroke, cardiac surgery, or joint replacement — who require intensive physical, occupational, or speech therapy before returning home.
Long-term care residents are individuals with chronic, progressive, or medically complex conditions — advanced heart failure, end-stage renal disease, or advanced dementia — who require indefinite nursing supervision.
Short-term and long-term residents may share the same licensed facility, but their care goals, therapy schedules, Medicare coverage timelines, and discharge expectations differ fundamentally.
Sadie G. Mays Health & Rehabilitation Center provides skilled nursing care alongside licensed physical therapy, occupational therapy, and speech-language pathology services from its campus in Atlanta’s Vine City neighborhood.
An assisted living community is a state-licensed residential care setting that provides structured support with activities of daily living — bathing, dressing, grooming, meal service, medication reminders, and housekeeping — for seniors who are medically stable but no longer able to live independently without daily assistance.
Assisted living communities are not medical facilities. Assisted living communities do not require a registered nurse on every shift, do not hold Medicare certification for skilled nursing services, and are not licensed to manage medically complex residents who require clinical intervention.
The Georgia Department of Community Health’s Healthcare Facility Regulation division licenses assisted living communities and personal care homes under separate regulatory frameworks with different staffing, disclosure, and service requirements. A personal care home and an assisted living community are not the same license category in Georgia.
Families must verify the specific license type of any community under consideration before placement, because the scope of care each license authorizes differs materially.
The strongest candidates for assisted living placement are seniors who are ambulatory or mobile with assistive devices, medically stable with well-controlled chronic conditions, and primarily in need of daily task supervision rather than licensed clinical intervention.
Georgia-licensed assisted living communities must discharge any resident whose medical needs exceed the scope of the community’s license — so families who confirm discharge policies before placement avoid disruptive emergency transfers when a resident’s condition escalates.
If you’re ready to get started, call us now!
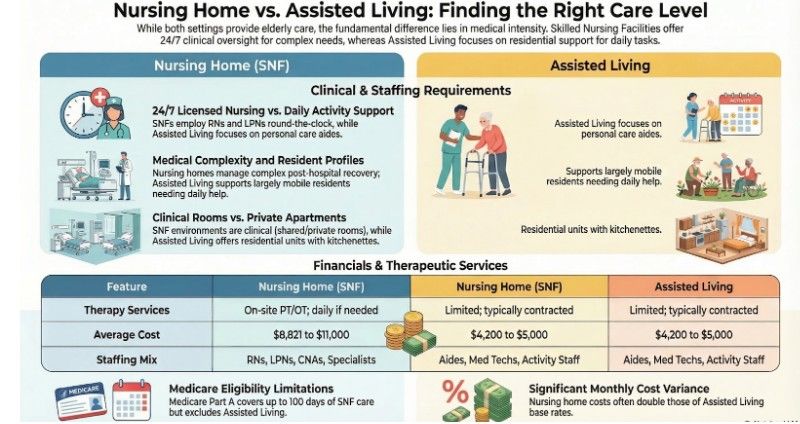
Staffing composition separates the two settings more than any other variable. Skilled nursing facilities employ RNs, LPNs, and CNAs on every shift around the clock.
Assisted living communities employ personal care aides and activity staff, with licensed nursing typically absent overnight. That gap determines which clinical conditions each setting can safely manage.
| Feature | Nursing Home (SNF) | Assisted Living |
| Medical care | 24/7 licensed nursing, physician oversight | Personal care aides; no RN required on shift |
| Staffing | RNs, LPNs, CNAs, therapists, specialists | Care aides, medication technicians, activity staff |
| Resident profile | Complex medical or post-hospital needs | Needs help with daily tasks; largely mobile |
| Environment | Clinical: shared or private room | Apartment-style, private unit with kitchenette |
| Therapy services | PT, OT, speech on-site; daily if needed | Limited; typically contracted and infrequent |
| Medicare covered? | Yes (Part A, up to 100 days post-hospital) | No (Medicaid waiver programs only) |
| Avg. monthly cost (Atlanta) | $8,821 to $11,000 | $4,200 to $5,000 (base rate) |
One distinction the table does not capture fully is therapy reimbursement. Medicare Part A covers therapy at up to five sessions per week in a certified skilled nursing facility.
The same therapy delivered within an assisted living community is not reimbursable under Medicare Part A.
Seniors needing intensive post-hospital rehabilitation must enter a skilled nursing facility to access both the clinical frequency and the Medicare coverage their recovery requires.
A skilled nursing facility is the correct placement when documented clinical needs require daily licensed nursing intervention that an assisted living community is not licensed to provide. Six conditions reliably signal that skilled nursing is necessary:
| Clinical Indicator | Why Assisted Living Cannot Manage It |
| Active wound requiring RN assessment and dressing changes | Assisted living staff are not licensed to perform clinical wound care |
| Physician-ordered IV antibiotic or infusion therapy | IV therapy requires licensed nursing administration and monitoring |
| Mechanical ventilator dependency | Ventilator management requires respiratory therapy and RN oversight |
| Enteral feeding tube management | Tube feeding requires a licensed nursing assessment and documentation |
| Post-surgical recovery with daily vital sign monitoring | Assisted living does not provide scheduled clinical monitoring |
| Hospital discharge with a physician order for skilled nursing | A physician’s order specifies the required level of care |
Advanced congestive heart failure (NYHA Class III or IV), uncontrolled type 2 diabetes with wound complications, end-stage renal disease requiring dialysis coordination, and severe COPD with oxygen dependency each require daily clinical monitoring outside the licensed scope of assisted living.
The CMS Care Compare database lets Atlanta families compare skilled nursing facilities by star rating, RN hours per resident per day, and inspection history before a placement decision is forced by hospital discharge timing.
Medicare Part A covers skilled nursing rehabilitation for up to 100 days per benefit period following a qualifying three-day inpatient hospital stay. As of January 2026, Medicare pays in full for days 1 through 20 and requires a $217-per-day copay for days 21 through 100.
Medicare coverage for rehabilitation in Atlanta covers what happens when day 100 benefits are exhausted.
Three or more documented 911 calls, falls with injury, or unplanned hospitalizations within 12 months constitute clinical evidence that the current care level is insufficient. Skilled nursing facilities assign a licensed nurse to every shift, so deterioration is caught before it escalates.
Assisted living is appropriate for seniors who are medically stable, mobile with or without assistive devices, and primarily need structured daily task support rather than licensed clinical intervention.
The right candidate has no active physician order for skilled nursing, no daily clinical intervention requirement, and no documented emergency nursing need anticipated within 12 to 24 months.
| Candidate Profile | Assisted Living Fits | Skilled Nursing Needed Instead |
| Medication management | Needs reminders and technician oversight | Requires nurse-administered injections or IV therapy |
| Mobility | Ambulatory with or without an assistive device | Requires a two-person transfer or a mechanical lift |
| Medical stability | Well-controlled chronic conditions | Active wound, respiratory dependency, or dialysis |
| Cognitive status | Mild to moderate; can follow daily routines | Severe dementia with behavioral risk or elopement |
| Emergency risk | Staff response sufficient | Requires on-shift RN assessment capability |
Seniors who can no longer safely manage meals, medications, or personal hygiene without daily prompting are candidates for assisted living. Structured routines reduce fall risk, certified technician oversight reduces medication errors, and three scheduled daily meals ensure consistent nutrition.
5 signs it is time to consider long-term care help families confirm whether the threshold has been crossed.
The National Institute on Aging identifies social isolation as a documented risk factor for cognitive decline, late-life depression, and increased all-cause mortality in adults over 65.
Medically stable seniors living alone with signs of social withdrawal gain clinically meaningful benefit from assisted living placement even when physical care needs remain minimal.
Seniors with documented fall risk, medication mismanagement, or emergency response delays from living alone are strong assisted living candidates.
Staff respond to emergencies, administer medications, and conduct welfare checks — so residents retain apartment-style privacy while eliminating unmonitored safety gaps.
If you’re ready to get started, call us now!
Atlanta skilled nursing facilities charged $8,821 to $9,900 per month for a semi-private room and $9,500 to $11,000 per month for a private room in 2024, according to the Genworth 2024 Cost of Care Survey.
Atlanta assisted living communities charged $4,200 to $5,000 per month at base rate, with care-level fees for higher-need residents pushing total monthly costs to $5,500 or more.
The cost gap between the two settings — roughly $4,500 to $6,000 per month — reflects the clinical staffing differential: skilled nursing facilities employ licensed nurses on every shift, maintain dedicated rehabilitation gyms staffed by licensed therapists, and carry the regulatory overhead of dual Medicare and Medicaid certification.
| Care Setting | Room / Unit Type | Monthly Cost (Atlanta) | Annual Cost |
|---|---|---|---|
| Skilled Nursing Facility | Semi-private room | $8,821 to $9,900 | $105,852 to $118,800 |
| Skilled Nursing Facility | Private room | $9,500 to $11,000 | $114,000 to $132,000 |
| Assisted Living | Standard unit (base rate) | $4,200 to $5,000 | $50,400 to $60,000 |
| Assisted Living | With high care-level fees | $5,500 to $6,500 | $66,000 to $78,000 |
| Memory Care (AL-based) | Secured unit | $5,200 to $6,500 | $62,400 to $78,000 |
Medicare Part A covers skilled nursing rehabilitation only. Medicare Part A does not cover assisted living placement under any circumstances.
Georgia Medicaid covers skilled nursing facility placement for residents who meet clinical need criteria and financial eligibility thresholds — income below approximately $2,829 per month and countable assets below $2,000 as of 2025.
Georgia’s Community Care Services Program (CCSP) Medicaid waiver funds assisted living placements for eligible individuals, but the CCSP operates at limited capacity, with active waitlists in the Atlanta metro area. The table below maps each payment source to each care setting.
| Payment Source | Nursing Home | Assisted Living | Key Conditions |
|---|---|---|---|
| Medicare Part A | Yes (up to 100 days) | No | 3-day qualifying hospital stay; skilled need documented |
| Georgia Medicaid | Yes (ongoing) | Limited | Income under $2,829/mo; assets under $2,000 |
| CCSP Medicaid Waiver | No | Yes (if eligible) | Clinical and financial eligibility required; waitlists are common |
| Long-Term Care Insurance | Yes (most policies) | Yes (most policies) | Cannot perform 2+ ADLs or cognitive impairment diagnosis |
| VA Aid and Attendance | Yes | Yes | Veteran or surviving spouse; wartime service; income limits apply |
| Private Pay | Yes | Yes | No restrictions; most flexible; used until other funding activates |
Note: CCSP waiver enrollment is subject to program capacity. Contact the Georgia Division of Aging Services or a Georgia-licensed elder law attorney to confirm the current waitlist status in the Atlanta area.
A licensed physician assessment or a formal evaluation by a certified geriatric care manager — a health and human services professional credentialed by the Aging Life Care Association — produces the most reliable level-of-care recommendation available to Atlanta families.
Both professionals assess functional ability, medical complexity, fall risk, and cognitive status and generate a specific placement recommendation backed by clinical documentation.
Families who make this decision without clinical input frequently underestimate the complexity of care and place a loved one in a setting that cannot safely meet documented needs.
Use the five questions below to structure the family conversation before engaging a physician or geriatric care manager:
The step-by-step guide to finding long-term care in Atlanta covers the full process from needs assessment through facility selection and admission.
Not sure which level of care your loved one needs? Contact the Sadie G. Mays admissions team today for a free consultation and help identifying the right clinical and financial fit.
Skilled nursing facilities and assisted living communities serve clinically distinct populations. Placing a resident in the wrong setting creates an avoidable safety risk, unnecessary costs, or a loss of independence.
The placement decision belongs to the physician and the clinical record; first, family preference is a secondary factor.
Sadie G. Mays Health & Rehabilitation Center — a nonprofit SNF established in Atlanta in 1948 — provides skilled nursing care, short-term rehabilitation, long-term residential care, hospice care, and respite care. Schedule a tour to meet the clinical team and review current pricing.
A skilled nursing facility provides 24-hour licensed nursing care for medically complex residents. An assisted living community provides help with daily activities in a residential setting without RN-level medical supervision on every shift. The distinction is documented clinical need, not age or preference.
Medicare does not cover assisted living under any circumstances. Medicare Part A covers only short-term skilled nursing rehabilitation. Georgia’s CCSP Medicaid waiver funds assisted living for financially and clinically eligible individuals, but program capacity is limited, and waitlists in the Atlanta area are common.
If a parent requires daily nursing intervention — wound care, IV therapy, medication titration, or post-surgical monitoring — a skilled nursing facility is appropriate. If the primary need is help with bathing, meals, and daily activities in a supervised setting, assisted living is the correct placement level.
Yes. Georgia regulations require an assisted living community to discharge any resident whose medical needs exceed the community’s licensed scope of care. Families should confirm the facility’s discharge policy and transfer-coordination process before placement, so that a care escalation does not become an emergency transition.
Atlanta skilled nursing facilities cost $8,821 to $11,000 per month versus $4,200 to $5,000 per month for assisted living base rates — a gap of $4,500 to $6,000 per month. The cost difference reflects the licensed nursing staffing and Medicare and Medicaid regulatory infrastructure that a skilled nursing facility must maintain.